
 June Roberts
June Roberts 
When to refer people with asthma to a specialist – using the Advanced Access Collaborative (AAC) pathway and HASTE tool
For many people, asthma can be well managed in primary care. But for some, symptoms remain difficult to control. This can mean frequent exacerbations, hospital visits, or ongoing problems despite the optimal treatment.[1] For these patients, getting specialist input can make a real difference, but the challenge for primary care teams is knowing when to refer.
Why referral matters
As asthma becomes more complex—with different phenotypes, more comorbidities, and new treatment options such as biologics—it’s vital that primary care teams stay alert to those patients who may need specialist input. Asthma UK estimates that around 200,000 people in the United Kingdom live with severe asthma, meaning their condition requires high-dose treatment or remains uncontrolled despite it — yet, only about 18% are referred to the appropriate services.[1] Delaying referral not only risks unnecessary hospital admissions, but can also reduce quality of life and increase mortality risk.[2]
Specialist services can offer patients more than what’s available in routine care. Referral can unlock access to:[3][4]
Advanced tests – such as bronchial challenge testing, induced sputum analysis, FeNO testing, and allergy investigations
Biologic therapies – treatments like anti-IgE, anti-IL5, and anti-IL4R agents. It’s thought that around 60,000 people could benefit, but fewer than 11,000 are currently receiving them
Multidisciplinary care – input from respiratory nurses, physiotherapists, pharmacists, and psychologists
Tailored plans – personalised management based on asthma type and comorbidities
Spotting uncontrolled asthma
The AAC pathway gives clear criteria for identifying uncontrolled asthma. Key indicators include:[3]
- Two or more exacerbations per year needing oral corticosteroids (OCS), or one or more serious episodes leading to hospital or emergency department attendance
- An exacerbation is defined as three or more days of OCS, or an increase in OCS dose (if already on maintenance) for at least three days
- Poor day-to-day control: frequent reliever use, night waking, or activity limited by asthma. The Asthma Control Test (ACT) is a useful tool here
- Six or more prescriptions for a short-acting beta2 agonist (SABA) in a year
Patients can be identified up at:[3]
- Their annual review
- A visit following an exacerbation
- Through proactive searching of patient records
Referral should also be considered if a patient is on long-term maintenance OCS (≥5 mg prednisolone daily for three months or more), or if they’ve previously been admitted to intensive care.[3]
Optimising care in primary care
Before referral, it’s important to make sure all the basics have been covered in primary care. This step is about giving patients the best chance of achieving control before moving on to specialist care.[3]
Key elements of optimisation in primary care include:[3]
- Checking the diagnosis and reviewing test results (FeNO, spirometry, peak flow, blood eosinophils)
- Looking for comorbidities such as allergic rhinitis, gastro-oesophageal reflux, COPD, anxiety, or breathing pattern problems
- Reviewing inhaler technique
- Confirming adherence, especially to inhaled corticosteroids (ICS)
- Stepping up treatment according to national guidance, while avoiding routine use of maintenance OCS
- Ensuring the patient has a written or digital personalised self-management plan
- Supporting lifestyle changes such as smoking cessation, weight management, and exercise
- Considering social and psychological factors that might affect control
If the patient is still uncontrolled after optimisation, referral should be made within six months from the initial asthma consultation.[3]
Patient referral — using the HASTE tool
The AAC suggests using the HASTE checklist to make referral decisions clearer. If the patient is still struggling and you can tick off the HASTE points, it’s time to think about referral to secondary care or a severe asthma centre (Figure 1).[3]
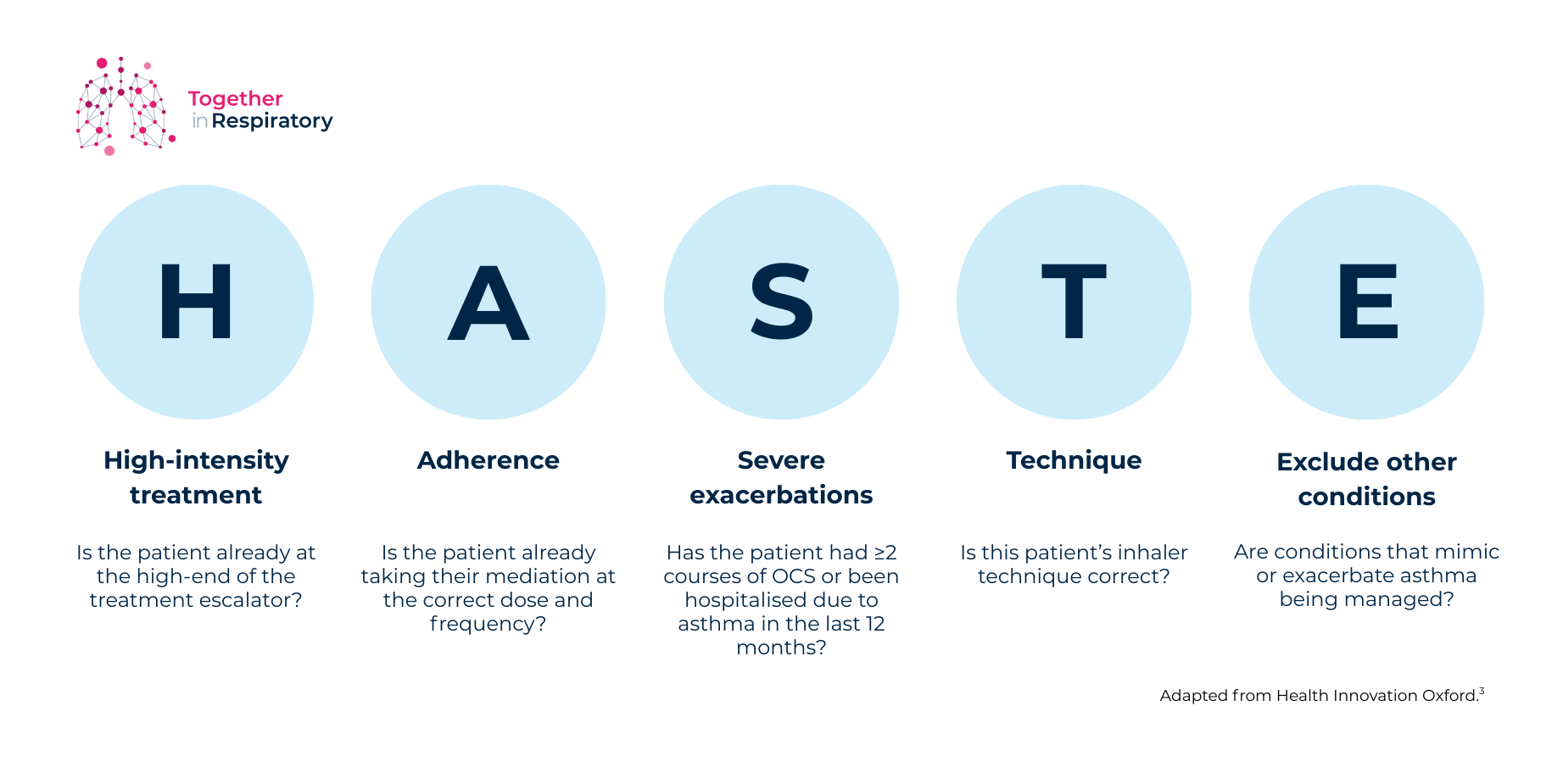
Figure 1: The HASTE tool.
When referring patients, it’s important to consider the content of the referral letter.
A good referral letter should include:[3]
- Why the patient is being referred
- Their current and previous asthma treatments
- The number of OCS courses, hospital admissions, and emergency department visits in the past year
- The number of ICS inhalers prescribed in the past year
- Any relevant comorbidities
- Relevant test results (with dates) e.g. spirometry, PEFR monitoring, blood eosinophil count, and FeNO
- Smoking history and body mass index (BMI)
Special considerations:
In addition to the HASTE tool, referral should be considered in the following situations:[2][5]
- The diagnosis isn’t clear, or another condition is suspected
- Occupational asthma is a possibility
- The patient is frequently seen in unscheduled care
- Psychosocial factors, such as housing or mental health, affect control
Paediatric considerations:
In children, poor response to treatment often has a simple explanation such as poor inhaler technique, poor adherence, or environmental factors like damp housing or second-hand smoke. These should be checked first, along with alternative diagnoses.[5]
If none explain the problem, referral to paediatric respiratory services is recommended. Children with at least one hospital admission or two or more emergency department visit for asthma in 12 months should always be referred.[5]
Concluding thoughts:
Timely referral can make a huge difference to people living with asthma. It can reduce hospital admissions, improve quality of life, and open up access to treatments that may transform outcomes.[1][2][3]
The AAC pathway and HASTE checklist give primary care teams clear, practical tools to support decision-making. And while optimisation in primary care is essential, it’s worth remembering that when in doubt, seeking specialist advice is rarely the wrong move.[1][2][3]
Abbreviations:
AAC, Advanced Access Collaborative; ACT, Asthma Control Test; BMI, body mass index; COPD, chronic obstructive pulmonary disease; ED, emergency department; FeNO, fractional exhaled nitric oxide; HASTE, Holistic Assessment, Symptoms, Treatment, Exacerbations; ICS, inhaled corticosteroid; IgE, immunoglobulin E; IL4R, interleukin-4 receptor; IL5, interleukin-5; OCS, oral corticosteroids; PEFR, peak expiratory flow rate; SABA, short-acting beta2 agonist.
References:
[1] Primary Care respiratory update. Available at https://www.pcrs-uk.org/sites/default/files/2022-December-25-SevereAsthmaPragGuide-Clinical.pdf. Accessed September 2025
[2] Price D, et al. Asthma referrals: a key component of asthma management that needs to be addressed. J Asthma Allergy. 2017;10:209–223
[3] Health Innovation Oxford. Available at https://www.healthinnovationoxford.org/wp-content/uploads/2022/06/AAC-Pathway-16.9_FINAL-No-NHS.pdf. Accessed September 2025
[4] Health Innovation Oxford. Available at https://www.healthinnovationoxford.org/wp-content/uploads/2022/01/SA-Toolkit.pdf. Accessed September 2025.
[5] NICE [NG245]. Available at https://www.nice.org.uk/guidance/ng245/resources/asthma-diagnosis-monitoring-and-chronic-asthma-management-bts-nice-sign-pdf-66143958279109. Accessed September 2025.

Subscribe to the newsletter
Get started
Related Stories

Everyone's Talking About
The importance of identifying palliative care needs in our patients with COPD
Read article
